| |
| |
 5年奥希还是复发了,伴有恶性胸水该
家母2020年直接开始服用奥西替尼,效果一直很好,最近两个月出现胸水以及锁骨淋巴肿大
5年奥希还是复发了,伴有恶性胸水该
家母2020年直接开始服用奥西替尼,效果一直很好,最近两个月出现胸水以及锁骨淋巴肿大
 庄莉教授、陈雄教授:不同癌种MET变
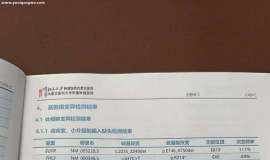
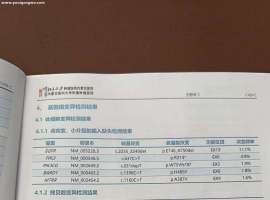
整理者:雨过天晴审核人:鹰版为帮助MET基因异常等少见靶点NSCLC患者解决在治疗过程中
庄莉教授、陈雄教授:不同癌种MET变
整理者:雨过天晴审核人:鹰版为帮助MET基因异常等少见靶点NSCLC患者解决在治疗过程中
 依沃西单抗肺癌一线适应症获批!全球
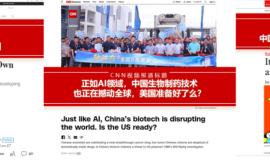
转载自:良医汇患者指南2025年4月25日,国家药监局官网发布重磅消息:我国自主研发的
依沃西单抗肺癌一线适应症获批!全球
转载自:良医汇患者指南2025年4月25日,国家药监局官网发布重磅消息:我国自主研发的
 【免疫组化结果已出】想咨询了解一下
性别:男
年龄:73岁
基础班:高血压
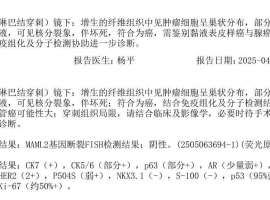
目前身体状况:右侧锁骨上有肿块并伴随痛感;咳
【免疫组化结果已出】想咨询了解一下
性别:男
年龄:73岁
基础班:高血压
目前身体状况:右侧锁骨上有肿块并伴随痛感;咳
 去除化疗,沿用A+T治疗咨询帖
本人父亲想去除化疗,沿用A+T的治疗方案,大概有以下几点原因:
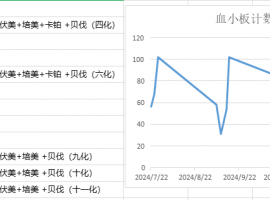
1 培美副作用导致的骨
去除化疗,沿用A+T治疗咨询帖
本人父亲想去除化疗,沿用A+T的治疗方案,大概有以下几点原因:
1 培美副作用导致的骨







 显身卡
显身卡