жң¬её–жңҖеҗҺз”ұ иҖҒ马 дәҺ 2012-5-10 00:41 зј–иҫ‘
5. A phase II study of daily afatinib (BIBW 2992) with or without temozolomide (21/28 days) in the treatment of patients with recurrent glioblastoma.
Meeting:
2011 ASCO Annual Meeting
Abstract No:
2010
Citation:
J Clin Oncol 29: 2011 (suppl; abstr 2010)
Author(s): D. D. Eisenstat, L. B. Nabors, W. P. Mason, J. R. Perry, W. R. Shapiro, P. Kavan, S. Phuphanich, Y. Fu, X. J. Cong, M. Shahidi, D. A. Reardon; CancerCare Manitoba, University of Manitoba, Winnipeg, MB, Canada; University of Alabama at Birmingham, Birmingham, AL; Princess Margaret Hospital, University of Toronto, Toronto, ON, Canada; Sunnybrook Health Sciences Centre, Toronto, ON, Canada; St. Joseph's Hospital and Medical Center, Phoenix, AZ; McGill University and Segal Cancer Centre, Jewish General Hospital, Montreal, QC, Canada; Cedars-Sinai Medical Center, Los Angeles, CA; Boehringer Ingelheim, Ridgefield, CT; Boehringer Ingelheim, Bracknell, United Kingdom; Duke University Medical Center, Durham, NC
Abstract Disclosures
Abstract:
Background: Epidermal growth factor receptor (EGFR) is over-expressed in ~50% of glioblastoma (GBM); approximately half express the constitutively active mutant receptor EGFRvIII. Afatinib (A), an irreversible erbB family blocker (including EGFRvIII), has high levels of in vitro activity in tumor cell lines resistant to reversible EGFR inhibitors.Temozolomide (T) can overcome O6-methylguanine methyltransferase (MGMT) resistance. We hypothesized that daily A or daily A+T (AT, 21/28 days) may be an effective treatment for recurrent GBM. Methods: The trialвҖҷs primary objectives were to evaluate efficacy and safety of A and AT compared to T in recurrent GBM, and to assess molecular determinants of response to A. Patients (pts) with histologically-confirmed GBM at first recurrence after prior combined chemoradiotherapy were randomized 1:1:1 to receive A, AT or T. Randomization was stratified by age (вүӨ50 vs. >50 years) and Karnofsky Performance Status (KPS; 70, 80 vs. 90, 100). A was dosed daily at 40 mg; T was dosed at 75 mg/m2 for 21/28 days. The primary endpoint was 6-month progression-free survival rate (PFS-6). Independent imaging and pharmacokinetic assessments were obtained. Archival tumor samples were assessed for EGFR, EGFRvIII, PTEN, pAKT and MGMT. Patients were treated until undue toxicity or disease progression. Results: Enrolment was completed in June 2010. 119 pts were randomized (median age 58 years [range 22вҖ“81]) and 54% had a KPS of 70вҖ“80. The most frequent AEs in pts A-treated pts were diarrhea (70% and 68% in A and AT, respectively) and rash (80% and 69%). PFS-6 by investigator assessment was 3%, 17% and 22% in the A, AT and T arms, respectively. A was statistically worse compared to T (p=0.008); AT was comparable to T (p =0.59). Best overall response included partial response in one, five and six pts and SD in 22, 20 and 21 pts in A, AT and T, respectively. Preliminary biomarker data in 54 pts suggested durable disease control in EGFRvIII-positive pts treated with A/AT. Updated biomarker data will be presented. Conclusions: Afatinib has limited single-agent activity in recurrent GBM; however, potential activity in biomarker-selected pts warrants further evaluation.
дёҖе…ұжңү119еҗҚз—…дәәпјҢжҢү1пјҡ1пјҡ1еҲҶз»„пјҢдёҙеәҠз»“жһңиЎЁжҳҺпјҢ2992еҚ•иҚҜз»„зҡ„жңүж•ҲзҺҮзј“и§Јдәәж•°жҳҜ1дәәпјҢиҒ”еҗҲз»„жҳҜ5дәәпјҢжӣҝиҺ«жҺӘиғәз»„жҳҜ6дәәпјӣпјҢ2992еҚ•иҚҜз»„зҡ„зЁіе®ҡдәәж•°жҳҜ22дәәпјҢиҒ”еҗҲз»„жҳҜ20дәәпјҢжӣҝиҺ«жҺӘиғәз»„жҳҜ21дәәгҖӮ
иҜҙжҳҺ2992еҚ•иҚҜеҜ№иғ¶иҙЁзҳӨзҡ„ж•ҲзҺҮиҝҳжҲҗпјҢдҪҶжҜ”жӣҝиҺ«жҺӘиғәе·®дёҚе°‘пјҢиҖҢ2992иҒ”еҗҲжӣҝдёҺжӣҝеҚ•иҚҜжІЎжңүеҢәеҲ«гҖӮ
|



 зҲёзҲёжҷҡжңҹиӮәзҷҢиӮҝзҳӨе·Із»ҸзңӢдёҚеҲ°дәҶпјҒжҲ‘зЎ®
и®Іиҝ°иҖ…пјҡйҷҲе…Ҳз”ҹж•ҙзҗҶиҖ…пјҡpear
йҖӮйҖўжҡ‘еҒҮеҫ—й—ІпјҢжҲ‘еёҰзқҖ全家иҮӘй©ҫеҮәжёёпјҢжӯЈе°ҶжңҖеҗҺдёҖ件иЎҢжқҺеЎһ
зҲёзҲёжҷҡжңҹиӮәзҷҢиӮҝзҳӨе·Із»ҸзңӢдёҚеҲ°дәҶпјҒжҲ‘зЎ®
и®Іиҝ°иҖ…пјҡйҷҲе…Ҳз”ҹж•ҙзҗҶиҖ…пјҡpear
йҖӮйҖўжҡ‘еҒҮеҫ—й—ІпјҢжҲ‘еёҰзқҖ全家иҮӘй©ҫеҮәжёёпјҢжӯЈе°ҶжңҖеҗҺдёҖ件иЎҢжқҺеЎһ
 иӮәи…әзҷҢ10е№ҙпјҢдјҸзҫҺжӣҝе°ј еҝғиЎҖз®ЎеүҜдҪңз”Ё
еҘ¶еҘ¶78еІҒпјҢиӮәи…әзҷҢ10е№ҙпјҢ2017.7-2023.7第дёҖд»Јйқ¶еҗ‘иҚҜеҮҜзҫҺзәі6е№ҙпјҢ2023.7иҮід»ҠдјҸзҫҺжӣҝе°ј1е№ҙ
иӮәи…әзҷҢ10е№ҙпјҢдјҸзҫҺжӣҝе°ј еҝғиЎҖз®ЎеүҜдҪңз”Ё
еҘ¶еҘ¶78еІҒпјҢиӮәи…әзҷҢ10е№ҙпјҢ2017.7-2023.7第дёҖд»Јйқ¶еҗ‘иҚҜеҮҜзҫҺзәі6е№ҙпјҢ2023.7иҮід»ҠдјҸзҫҺжӣҝе°ј1е№ҙ
 вҖңиӮҫвҖқйҮҚиө·и§ҒпјҢжҠ—зҷҢд№ҹеҫ—дҝқиӮҫ
дҪңиҖ…пјҡй—ө
вҖңиӮқиӮҫеҠҹиғҪвҖқз»Ҹеёёиў«е’ұ们病еҸӢжҢӮеңЁеҳҙиҫ№пјҢжЈҖжҹҘзҡ„ж—¶еҖҷд№ҹжҳҜдёҖ并еҮәзҡ„жҠҘе‘ҠпјҢдҪҶз—…еҸӢ
вҖңиӮҫвҖқйҮҚиө·и§ҒпјҢжҠ—зҷҢд№ҹеҫ—дҝқиӮҫ
дҪңиҖ…пјҡй—ө
вҖңиӮқиӮҫеҠҹиғҪвҖқз»Ҹеёёиў«е’ұ们病еҸӢжҢӮеңЁеҳҙиҫ№пјҢжЈҖжҹҘзҡ„ж—¶еҖҷд№ҹжҳҜдёҖ并еҮәзҡ„жҠҘе‘ҠпјҢдҪҶз—…еҸӢ
 еҢ»е…»з»“еҗҲпјҡжү“йҖҡиӮҝзҳӨжӮЈиҖ…еұ…家иҗҘе…»вҖңжңҖ
ж•ҙзҗҶиҖ…пјҡйӣЁиҝҮеӨ©жҷҙиӮҝзҳӨжӮЈиҖ…зҡ„жІ»з–—дёҺеә·еӨҚжҳҜдёҖдёӘеӨҡз»ҙеәҰгҖҒзі»з»ҹжҖ§зҡ„е·ҘзЁӢпјҢиҖҢиҗҘе…»жІ»з–—жӯЈжҳҜе…¶
еҢ»е…»з»“еҗҲпјҡжү“йҖҡиӮҝзҳӨжӮЈиҖ…еұ…家иҗҘе…»вҖңжңҖ
ж•ҙзҗҶиҖ…пјҡйӣЁиҝҮеӨ©жҷҙиӮҝзҳӨжӮЈиҖ…зҡ„жІ»з–—дёҺеә·еӨҚжҳҜдёҖдёӘеӨҡз»ҙеәҰгҖҒзі»з»ҹжҖ§зҡ„е·ҘзЁӢпјҢиҖҢиҗҘе…»жІ»з–—жӯЈжҳҜе…¶
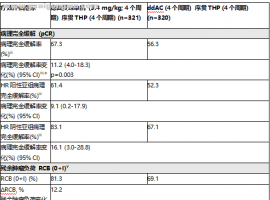 DESTINY-Breast11 IIIжңҹдёҙеәҠз ”з©¶
DESTINY-Breast11 IIIжңҹдёҙеәҠз ”з©¶пјҡдјҳиө«еҫ—еәҸиҙҜTHPж–№жЎҲжңҜеүҚжІ»з–—пјҢдҪҝй«ҳйЈҺйҷ©HER2йҳіжҖ§ж—©жңҹ
DESTINY-Breast11 IIIжңҹдёҙеәҠз ”з©¶
DESTINY-Breast11 IIIжңҹдёҙеәҠз ”з©¶пјҡдјҳиө«еҫ—еәҸиҙҜTHPж–№жЎҲжңҜеүҚжІ»з–—пјҢдҪҝй«ҳйЈҺйҷ©HER2йҳіжҖ§ж—©жңҹ




 жҳҫиә«еҚЎ
жҳҫиә«еҚЎ
