Abemaciclib data highlight Eli Lilly’s case on CDK 4/6 9 ^* ^9 I* _" `& u7 m0 L4 Y% h
. v# H; v7 Y3 a8 V& TCan Eli Lilly’s ($LLY) CDK 4/6 inhibitor abemaciclib still make a splash after Pfizer ($PFE) grabbed the pioneering OK in the field for palbociclib (Ibrance) and Novartis ($NVS) has touted a promising early end to their pivotal study for ribociclib?9 H+ G' `# c2 _; v7 @5 o
9 s& r3 B) W5 t8 d' NThe next big turning point on that front is looming as analysts look to see if Lilly can wrap its key franchise trial early as well. But a new Phase I study covering a range of cancers and published in Cancer Discovery underscores some of the reasons the FDA decided to hand out “breakthrough” status on abemaciclib. And it also highlights reasons why this drug still has potential to differentiate itself and vault ahead of its major league rivals.2 [% g. S/ {* |
- R3 y0 |& B+ m: w9 c' P9 v: O
CDK 4/6 inhibitors like abemaciclib are designed to block a key pathway in cell proliferation that runs amok when cancer takes root. Block that process early enough, and a drug can arrest a whole cascade of events that help drive cancer.
) T* _8 F* V# s: G# C, u
. h/ A' W0 f8 E2 d" a. r; UThe key takeaways from the Lilly study: Unlike the two rivals, which are typically dosed three weeks on and one week off to manage the dose-limiting toxicity of neutropenia for their drugs, abemaciclib’s red flag is for severe fatigue, allowing for continual dosing. Prominent researchers in the study also highlight that Lilly’s drug apparently hits CDK 4 harder than 6, possibly sparing white blood cells. This may help explain why their drug has been able to score more significant data as a monotherapy than the rivals, which are provided as a combo with hormonal therapy.
# i& z$ h6 x1 _' F6 v7 [4 y4 } D( {) y; p. |# l' K
“For the other two agents (palbociclib and ribociclib), the (single agent) response rates are low with these drugs,” says Dana Farber investigator Geoffrey Shapiro, who’s done work on all three big CDK 4/6 inhibitors.
" |5 i7 l3 R9 Z0 t6 n( O0 a' v c* d
7 T1 h$ K; y6 p; {. H" j# z“We have a fairly hefty response rate for hormone receptor-positive cancer. That’s a bit of a difference,” he adds, and perhaps a key reason why the FDA handed out the breakthrough title, which is intended to help facilitate the development process.' U a6 y; @6 o3 @- a
* p6 d7 D3 L% u8 VTo be sure, says Shapiro, much of what they’re still learning about abemaciclib is preliminary. Hammering away at CDK 4/6 continuously may improve efficacy, he notes, but it may also turn out that constant inhibition may actually encourage resistance, forcing the cancer to find a new pathway. On/off dosing might be able to avoid that, but a lot more work needs to be done before that point can be determined.) J% D4 f0 w$ t; G" c9 z0 T Z
/ P. K( C _9 i x1 H6 @1 |Researchers recruited 225 patients for this study. In the expansion phase, abemaciclib was administered as a single agent to 47 patients with breast cancer, 68 with non-small cell lung cancer, 17 with glioblastoma, 26 with melanoma and 15 with colorectal cancer.- v P% ~5 m, Z ]+ c
6 C! }; K" z; a9 ^0 x8 D' e
Lilly was looking for a better idea of which patients would be most likely to respond and uncovered several key signs for hormone-receptor positive breast cancer and KRAS-mutant NSCLC.! [$ d M# h- U2 E+ \, X
" p1 q' G ?: A+ o& |. P0 lOut of the 36 hormone receptor-positive breast cancer cases, 11 had a partial response while 18 patients had stable disease. Among 68 patients with NSCLC, there were only two partial responses and 31 cases of stable disease. Significantly, one of the partial responses and 12 instances of stable disease involved KRAS-mutant NSCLC.6 i# q' q* a! c2 d
0 F5 c* v/ _6 ]( m
In breast cancer, the median PFS for the entire population was 5.8 months, Shapiro reports. The median PFS for the hormone receptor-positive population was 8.8 months." ?$ G3 y) I1 V' I
( r* H, C4 h: q. d/ Z“All breast cancer patients who achieved RECIST response (The Response Evaluation Criteria In Solid Tumors for judging a response) were hormone-receptor positive. Among these patients, the median duration of response was 13.4 months.
7 Z& @5 _! ^9 W( q' |2 P# [# ^% U+ b! p% k2 |! G
In lung cancer: Among patients with tumors harboring KRAS mutation, 9 out of the 29 had a PFS rate greater than 24 weeks (6 months). “Among patients with KRAS wild type tumors, 4/33 had PFS > 24 weeks (6 months). Also, of 4 patients who received abemaciclib > 12 months, 3 had tumor harboring KRAS mutation.& |5 a3 n: F$ K" o* A, l3 g- u
, T, l J& ~7 c+ Q T( N$ X“It is noteworthy that KRAS mutated lung cancer is subdivided into KRAS alone,” noted Shapiro, “KRAS with concomitant TP53 mutation and KRAS with concomitant LKB1 (STK11) loss. KRAS/LKB1 predicts an especially aggressive phenotype. Tumor regressions were noted across these subdivisions of KRAS mutant lung cancer.
9 @: z. W+ k) a; I# t/ n1 {- U. F; N) o3 ~) m9 c/ e
“So, although more work needs to be done to truly identify the lung cancer population most likely to benefit from abemaciclib monotherapy, these data in KRAS mutant disease are very promising.: z2 ^# o6 _* V3 u- {2 c5 C: E% a
* H r7 w6 U9 P8 b/ X; {5 d2 }, v“Finally, for your question about ‘what did we learn, or ‘what was surprising or confirmed,’” adds Shapiro, “it is noteworthy that we confirmed preclinical models indicating abemaciclib can cross the blood brain barrier. Among glioblastoma patients, cerebrospinal fluid concentrations approximated those in plasma, and 2 glioblastoma patients have achieved very long term benefit on abemaciclib.”
, R" E) n( e" g; u& _. _4 h' `
' J t0 c+ c" F* t' o2 dProvided the data hold up in the first pivotal study, an approval for Eli Lilly is almost assured. The FDA understands this mechanism well, has been working with three big players that have devoted significant resources to the trials and gave breakthrough status to Pfizer and Lilly to help hurry things along.' B9 q: C0 A; I6 `* E R3 P/ J) l
8 m. b$ l- R D" S5 C( e1 q
Whether Lilly can make the big jump to top contender for this blockbuster market, though, remains to be seen. And Pfizer’s investigators haven’t hesitated to counter that abemaciclib could have severe gastrointestinal issues.
3 Z% x6 c, K* |2 {: ~. t
5 b. q/ ^6 [8 f1 L6 }' SWith billions at stake, all the stops are being pulled out.8 q f7 ?- ^5 A* s
) e4 j# U) r T) r0 b/ h+ I3 O6 U6 G! ^/ d2 \
http://www.fiercebiotech.com/abe ... lting-ahead-cdk-4-6 |
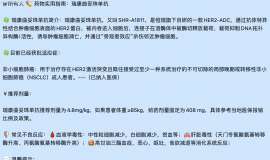
 汇总4月最新:临床试验招募| 小细胞
"化疗±免疫后进展了,还能怎么办?"——这是许多小细胞肺癌患者和家属的困境。
临
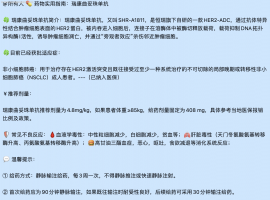
汇总4月最新:临床试验招募| 小细胞
"化疗±免疫后进展了,还能怎么办?"——这是许多小细胞肺癌患者和家属的困境。
临
 新人求助
我爸爸身体不适 26 年 4 月 10 号去医院检查,初步结果是肺肿可能是肺癌,因年纪大 7
新人求助
我爸爸身体不适 26 年 4 月 10 号去医院检查,初步结果是肺肿可能是肺癌,因年纪大 7
 母亲肺腺癌晚期骨转移,EGFR21突变,
母亲1970年出生,56周岁,身高163cm,体重98kg(196斤)。2025年9月23日肺炎住院,胸
母亲肺腺癌晚期骨转移,EGFR21突变,
母亲1970年出生,56周岁,身高163cm,体重98kg(196斤)。2025年9月23日肺炎住院,胸
 肺癌术后五年,脑膜转移治疗三年,伏
2025年8月14日更新: 终于输液港血培养结果为阴性了,14天美平消炎出院了,昨天开始双
肺癌术后五年,脑膜转移治疗三年,伏
2025年8月14日更新: 终于输液港血培养结果为阴性了,14天美平消炎出院了,昨天开始双
 从6个月到1400多天:一位晚期肺癌患
2026年全国肿瘤防治宣传周(4月15日-21日)即将到来,今年中国抗癌协会的主题是“肿瘤
从6个月到1400多天:一位晚期肺癌患
2026年全国肿瘤防治宣传周(4月15日-21日)即将到来,今年中国抗癌协会的主题是“肿瘤






 显身卡
显身卡